Just a quick post to announce that the hard drive on my computer has died. It will take a week or two to get everything fixed and transferred over, so I'll have less internet access until then. I'll be back to posting by the end of the month.
Always Double Check
On Sunday one of my associates saw a puppy who had swallowed some rocks. The abdominal radiographs showed the rocks clearly and one was somewhat large. Since the puppy was acting normal, she recommended that he come back the following day to repeat the x-rays and see if the rocks had passed through the gastrointestinal tract.
I saw him on Monday, repeated the radiographs, and noted that the larger stone and one other were still in his stomach. This was concerning because it should only take 2-3 hours for the stomach to empty and less than a day for everything to pass through the other end. Here were were a full day later and the rocks remained. This meant that we were going to have to go in surgically and remove them to prevent further problems. Since he was still acting normal I scheduled them for today and had them watch him overnight.
A principle I learned long ago is that when dealing with a GI foreign body that you plan to surgically remove, always double-check that it's still there just prior to surgery. So when the puppy came in this morning I took one more x-ray to make sure the rocks were still in the stomach. Lo-and-behold, the rocks had moved! They were out of the stomach and into the small intestine. And the puppy was still eating, active, and looking perfectly normal.
This is why we need to double-check in situations like this. If I had just jumped in and started the surgery not only would I have put him through it potentially unnecessarily, but the rocks wouldn't have been in the stomach where I would have looked. By a simple repeat of the radiographs I was able to save a surgery and the ensuing risks.
Now the puppy isn't completely out of the woods as he could still obstruct. But he's in good enough shape that we're going to give him another 48 hours and re-evaluate whether we need to do surgery at that point. And before we do, we'll definitely repeat radiographs one more time!
I saw him on Monday, repeated the radiographs, and noted that the larger stone and one other were still in his stomach. This was concerning because it should only take 2-3 hours for the stomach to empty and less than a day for everything to pass through the other end. Here were were a full day later and the rocks remained. This meant that we were going to have to go in surgically and remove them to prevent further problems. Since he was still acting normal I scheduled them for today and had them watch him overnight.
A principle I learned long ago is that when dealing with a GI foreign body that you plan to surgically remove, always double-check that it's still there just prior to surgery. So when the puppy came in this morning I took one more x-ray to make sure the rocks were still in the stomach. Lo-and-behold, the rocks had moved! They were out of the stomach and into the small intestine. And the puppy was still eating, active, and looking perfectly normal.
This is why we need to double-check in situations like this. If I had just jumped in and started the surgery not only would I have put him through it potentially unnecessarily, but the rocks wouldn't have been in the stomach where I would have looked. By a simple repeat of the radiographs I was able to save a surgery and the ensuing risks.
Now the puppy isn't completely out of the woods as he could still obstruct. But he's in good enough shape that we're going to give him another 48 hours and re-evaluate whether we need to do surgery at that point. And before we do, we'll definitely repeat radiographs one more time!
Veterinary Shortage
Believe it or not, here in the US there is a shortage of veterinarians. More specifically there is a shortage of vets entering large animal (livestock) medicine and public health medicine. This concern is frequently mentioned in industry journals and articles, and has become a real issue here. Fewer and fewer graduating vets are choosing to enter these fields of medicine, so as older practitioners retire there are less waiting to replace them.
In some parts of the country there is only one vet per 100,000 or more cattle. About 75% of newly graduated vets pursue a career in small animal medicine. I believe that this problem is related to the changing demographics of where people live. A century ago most people were from rural communities, growing up on or around farms. Nowadays the population is predominantly suburban or urban, like myself. I never had any exposure to or experience with farm animals until I was actually in veterinary school, and never considered going in this direction with my job. Since I had grown up around families and pets, I wanted to work with these animals and situations. This is common of most new vets and not many have farm experience.
The reason this shortage is a problem is that our food supplies are from animals, which require proper veterinary care. Without vets skilled in these areas of medicine the animals may suffer, be sick, or otherwise not be fit for consumption. The shortage actually puts public health and food supplies at risk. It's actually reached the point where the US Department of Agriculture is introducing legislation to give special grants to encourage people to pursue careers in the areas of shortages and change how veterinary schools select candidates.
So if anyone wants a job in veterinary medicine in the US and you want to work with farm animals, your career is virtually guaranteed!
In some parts of the country there is only one vet per 100,000 or more cattle. About 75% of newly graduated vets pursue a career in small animal medicine. I believe that this problem is related to the changing demographics of where people live. A century ago most people were from rural communities, growing up on or around farms. Nowadays the population is predominantly suburban or urban, like myself. I never had any exposure to or experience with farm animals until I was actually in veterinary school, and never considered going in this direction with my job. Since I had grown up around families and pets, I wanted to work with these animals and situations. This is common of most new vets and not many have farm experience.
The reason this shortage is a problem is that our food supplies are from animals, which require proper veterinary care. Without vets skilled in these areas of medicine the animals may suffer, be sick, or otherwise not be fit for consumption. The shortage actually puts public health and food supplies at risk. It's actually reached the point where the US Department of Agriculture is introducing legislation to give special grants to encourage people to pursue careers in the areas of shortages and change how veterinary schools select candidates.
So if anyone wants a job in veterinary medicine in the US and you want to work with farm animals, your career is virtually guaranteed!
Horner's syndrome, revisited, again
By far, this topic has received the most attention and comments on this blog. Many, if not most, cases of Horner's syndrome are idiopathic, meaning that no discernible causes can be found. Again, Horner's syndrome is not a disease per se, but rather a constellation of clinical signs that make up the syndrome: ptosis (or drooping eyelid), enophthalmos (or sinking in of the eyeball), miosis (constricted pupil), and prolapsed nictitans (presence of 3rd eyelid covering the eyeball more than usual).
When this young Cocker Spaniel was presented to me yesterday for an eye infection, she exhibited all signs of Horner's mentioned above. By default, because she's a Cocker Spaniel, I had a good look deep into her ear canal and lo and behold she had pretty convincing evidence of an ear infection, a ruptured ear drum, and likely a middle ear infection. X-rays of her middle ears were iffy, as they often are (CT is better for these little structures). We sedated her, flushed her ears with saline, cultured the "gunk", and sent her home on topical and oral antibiotics, and analgesics.
In this case, otitis media (an infection of the middle ear) is the likely culprit causing Horner's syndrome.

Not the Cocker Spaniel in question! The affected eye is evident.
When this young Cocker Spaniel was presented to me yesterday for an eye infection, she exhibited all signs of Horner's mentioned above. By default, because she's a Cocker Spaniel, I had a good look deep into her ear canal and lo and behold she had pretty convincing evidence of an ear infection, a ruptured ear drum, and likely a middle ear infection. X-rays of her middle ears were iffy, as they often are (CT is better for these little structures). We sedated her, flushed her ears with saline, cultured the "gunk", and sent her home on topical and oral antibiotics, and analgesics.
In this case, otitis media (an infection of the middle ear) is the likely culprit causing Horner's syndrome.

Not the Cocker Spaniel in question! The affected eye is evident.
A Time Bomb--Atlantoaxial Problems
I had a rather scary problem today, and one I've faced before. A terrier-mix had been having mysterious pain for a week or more. Another vet had taken radiographs and noted extensive fusing of many vertebrae in the spine, a condition called spondylosis. This certainly can cause pain, and I've seen those cases before. The dog was placed on two analgesics and sent home for observation. Unfortunately the pain didn't go away. The owner thought it was in the neck and not the back. Ironically, the only part of the spine that the other vet didn't get images of was the neck. It was also puzzling because the pain wasn't consistent or repeatable. When I examined the dog I manipulated the neck without any problems, resistance, or pain.
I've begun to appreciate modern technology in aiding a diagnosis, but not in the way many might think. One of the keys to this case was the video the owner took with her digital camera. Since the pain was sporadic and mainly happened at night, she took the video so a vet could see what was going on. The dog's posture and actions certainly seemed to indicate neck pain. But without symptoms in the clinic, this was puzzling. Well, we knew a problem was in the neck, so we took x-rays of that area.
When I looked at the film my breath caught. The problem was immediately obvious and was a serious one. This is an image of the neck of a normal dog.
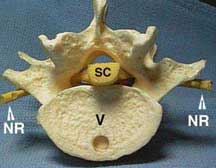
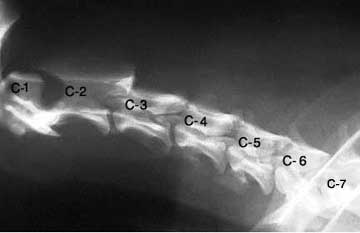 The first vertebrae (here labeled C-1) is the atlas and the second one (C-2) is the axis. The atlas articulates with the skull and supports the head. Most of the mobility of the head is going to come from the interactions of these two vertebrae with the skull. In the center of the vertebrae is a hollow tunnel through which the spinal cord runs (labeled "sc" below). In the above image the spinal cord would run where the letters and numbers are.
The first vertebrae (here labeled C-1) is the atlas and the second one (C-2) is the axis. The atlas articulates with the skull and supports the head. Most of the mobility of the head is going to come from the interactions of these two vertebrae with the skull. In the center of the vertebrae is a hollow tunnel through which the spinal cord runs (labeled "sc" below). In the above image the spinal cord would run where the letters and numbers are.
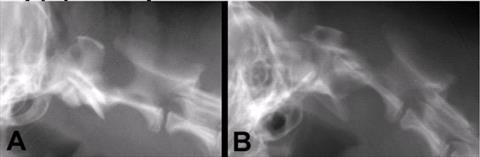
The left image is normal and the right one shows atlantoaxial subluxation. Pay careful attention to the center of the vertebrae where the spinal cord would run. The displacement of the vertebrae bends the spinal cord and puts pressure against it. This can cause pain and was the source of our problems.
The scariest part of this is that this dog is a ticking time bomb. At any time the dog's neck could shift more severely, immediately causing damage to the spinal cord. This can cause paralysis from the neck down, but more importantly can cause problems with the heart and respiratory system since the nerves controlling these vital organs run through the neck. I've seen a couple of cases like this and have always shuddered when I saw the radiographs because of the potential harm that could have happened during the exam. When a patient has neck pain we will manipulate and bend the neck in all directions to see if we can isolate where the problem is. Unfortunately in this case that manipulation can damage the spine.
Thankfully, this is a treatable problem. Surgery can be performed to place pins or plates between the vertebrae once they are realigned, keeping them from moving out of place again. Patients normally do well after this surgery and can lead normal lives afterwards. This dog has an appointment with a surgical specialist and will hopefully have the procedure done soon before this particular bomb goes off.
I've begun to appreciate modern technology in aiding a diagnosis, but not in the way many might think. One of the keys to this case was the video the owner took with her digital camera. Since the pain was sporadic and mainly happened at night, she took the video so a vet could see what was going on. The dog's posture and actions certainly seemed to indicate neck pain. But without symptoms in the clinic, this was puzzling. Well, we knew a problem was in the neck, so we took x-rays of that area.
When I looked at the film my breath caught. The problem was immediately obvious and was a serious one. This is an image of the neck of a normal dog.
This dog had a severe dislocation of the atlas and axis. Below is an image from the 'Net and not from this case, but my patient was very similar.
The left image is normal and the right one shows atlantoaxial subluxation. Pay careful attention to the center of the vertebrae where the spinal cord would run. The displacement of the vertebrae bends the spinal cord and puts pressure against it. This can cause pain and was the source of our problems.
The scariest part of this is that this dog is a ticking time bomb. At any time the dog's neck could shift more severely, immediately causing damage to the spinal cord. This can cause paralysis from the neck down, but more importantly can cause problems with the heart and respiratory system since the nerves controlling these vital organs run through the neck. I've seen a couple of cases like this and have always shuddered when I saw the radiographs because of the potential harm that could have happened during the exam. When a patient has neck pain we will manipulate and bend the neck in all directions to see if we can isolate where the problem is. Unfortunately in this case that manipulation can damage the spine.
Thankfully, this is a treatable problem. Surgery can be performed to place pins or plates between the vertebrae once they are realigned, keeping them from moving out of place again. Patients normally do well after this surgery and can lead normal lives afterwards. This dog has an appointment with a surgical specialist and will hopefully have the procedure done soon before this particular bomb goes off.
A Night At The Museum
In my area we have a local science museum, the Tellus, that has some cool events. Most recently they hosted their second annual "Night At The Museum". The premise was very similar to the movies of the same name. Various displays of historical people come to life at night and interact with the museum visitors. My wife and I participated as Jules Verne (me) and Amelia Earhart (my wife). Other people portrayed figures such as Henry Ford, Galileo, Marie Curie, the Wright Brothers, and Nicola Tesla. For the entire night we acted in character, pretending we were the various characters come to life. Since we were really "museum displays" we would periodically have to freeze in place as if we were manikins. There were also two people dressed as security guards and when they approached we would have to immediately become frozen. The guards really played up on this, dusting us off, shining flashlights in our eyes, and interacting with the guests.
Most of this was designed for kids, but the adults seemed to enjoy it as well. We would educate people about the lives and accomplishments of our characters, sign autographs, pose for pictures, and otherwise enjoy ourselves as we did a lot of in-character improvisational interaction. I've always loved Verne's stories and enjoyed learning more about his life (he was born on February 8th, the same birthday as my father...he was friends with Alexander Dumas...he was a stickler for scientific accuracy in his stories). My wife has always been fascinated with Earhart and jumped at the chance to pretend to be her.
All of this was a big success, and it seems pretty certain that the Tellus Museum will do it again next year. If they do, I'm certainly going to participate again!
 My lovely wife as the spunky Amelia Earhart. Unfortunately you can't tell as well in this photo, but she looked really good.
My lovely wife as the spunky Amelia Earhart. Unfortunately you can't tell as well in this photo, but she looked really good.
 She's second from the left here. "Sally Ride" is in the blue jumpsuit in the middle with Henry Ford in the trenchcoat next to her and Tesla just to the right of him.
She's second from the left here. "Sally Ride" is in the blue jumpsuit in the middle with Henry Ford in the trenchcoat next to her and Tesla just to the right of him.
 Me as Jules Verne signing autographs. I'm next to a model of the interior if the earth, purposefully done because of Journey to the Center of the Earth.
Me as Jules Verne signing autographs. I'm next to a model of the interior if the earth, purposefully done because of Journey to the Center of the Earth.
 One of the guards making sure everything was okay with the Verne "manikin". I had to try and remain completely still and worked not to blink very much. There was one time where I was motionless for over five minutes and my contacts began to dry out.
One of the guards making sure everything was okay with the Verne "manikin". I had to try and remain completely still and worked not to blink very much. There was one time where I was motionless for over five minutes and my contacts began to dry out.
 Here I am next to Madame Marie Curie, Albert Einstein, a miner, and a chemist. Some people played non-specific characters such as chemists, paleontologists, and so on.
Here I am next to Madame Marie Curie, Albert Einstein, a miner, and a chemist. Some people played non-specific characters such as chemists, paleontologists, and so on.
Okay, so none of this was related to veterinary medicine, but it sure was fun!
Most of this was designed for kids, but the adults seemed to enjoy it as well. We would educate people about the lives and accomplishments of our characters, sign autographs, pose for pictures, and otherwise enjoy ourselves as we did a lot of in-character improvisational interaction. I've always loved Verne's stories and enjoyed learning more about his life (he was born on February 8th, the same birthday as my father...he was friends with Alexander Dumas...he was a stickler for scientific accuracy in his stories). My wife has always been fascinated with Earhart and jumped at the chance to pretend to be her.
All of this was a big success, and it seems pretty certain that the Tellus Museum will do it again next year. If they do, I'm certainly going to participate again!





Okay, so none of this was related to veterinary medicine, but it sure was fun!
An Emergency Repair
Being a vet can teach you unexpected skills and bring unexpected dangers. Here's a typical case....
Last week one of my techs was trying to restrain an unruly dog. He wasn't aggressive, just very wiggly and didn't want to stay still. We did what we needed to do with him, but she had difficulty getting him still enough and he kept trying to get out of her hold. She managed to pick up a few new bruises and some minor scratches. But one of the worst things that happened was that the dog got a foot in the pocket of her scrub top and tore the stitches from a corner.
Okay, so it wasn't a life-threatening problem. And it was only the corner of the pocket. But that's where the unexpected skills came into play. I didn't want her to spend the rest of the day with a dangling pocket, so I got to work. I've removed spleens, kidneys, and bladder stones and do surgery several days per week. So I pulled out a pack of suture, some needle holders, and started a "laceration repair".

Dark purple suture doesn't show up well against navy blue scrubs, so it isn't easy to tell. A simple continuous suture line and a few minutes later and the pocket was as good as new. And believe it or not this isn't the first time I've performed this particular procedure. I've sutured my lab coat pockets on more than on occasion.
Yet another unexpected life skill learned by being a vet.
Last week one of my techs was trying to restrain an unruly dog. He wasn't aggressive, just very wiggly and didn't want to stay still. We did what we needed to do with him, but she had difficulty getting him still enough and he kept trying to get out of her hold. She managed to pick up a few new bruises and some minor scratches. But one of the worst things that happened was that the dog got a foot in the pocket of her scrub top and tore the stitches from a corner.
Okay, so it wasn't a life-threatening problem. And it was only the corner of the pocket. But that's where the unexpected skills came into play. I didn't want her to spend the rest of the day with a dangling pocket, so I got to work. I've removed spleens, kidneys, and bladder stones and do surgery several days per week. So I pulled out a pack of suture, some needle holders, and started a "laceration repair".
Dark purple suture doesn't show up well against navy blue scrubs, so it isn't easy to tell. A simple continuous suture line and a few minutes later and the pocket was as good as new. And believe it or not this isn't the first time I've performed this particular procedure. I've sutured my lab coat pockets on more than on occasion.
Yet another unexpected life skill learned by being a vet.
Bye-Bye Eye
Most of the surgeries veterinarians perform are spays and neuters and are very routine. But it's not uncommon to do more advanced and uncommon procedures. Monday was one such surgery, as I removed a dog's eye, a surgery called "enucleation".
The dog is an old poodle who had a history of eye problems. His left eye had been injured many years ago and was shrunken and useless. His right eye had developed a cataract, so he was essentially blind. Last week the right eye suddenly became worse and the eye protruded. Apparently the globe (eyeball) had slightly popped out and the eyelids had slid behind it, trapping the eye in front of the lids. Infection developed and this was extremely painful. There was no saving the eye so the decision was made to remove it.
**WARNING!!!!!** If you're squeamish don't scroll down through the rest of the blog. I'm posting some pretty graphic images.
This is what the eye looked like just prior to surgery and after shaving and surgical prep. He is already under anesthesia at this point.



The cloudiness of the eye is a combination of cataract and pus. The dog was completely blind, so the eye was only causing discomfort. There was also severe damage to the eye so there wouldn't have been any benefit to putting it back into position. The surgery is actually not very difficult and can be done by most general practitioners. It's simply a matter of carefully cutting the muscles and connective tissues, gently freeing the globe from its attachments. After cutting the optic nerve at the back of the eye, the globe comes out easily.




The last photo is of the empty socket after the globe has been removed. The third eyelid and tear gland are removed and then the edges of the eyelid are cut away. The eyelids are sutured closed so that the socket and tissues are protected. In some cases a false eye is placed in the socket, but most vets don't do this and it is purely for appearances with no medical benefit. Here's a picture of the patient after the surgery was finished.

Dogs do quite well after the surgery and will go home with antibiotics and pain control. Sutures will come out in 7-10 days and by then they are usually back to normal. Since this kind of surgery is done because of severe damage to the eye, the dog is already blind prior to surgery, so removing the eye only improves their quality of life.
The dog is an old poodle who had a history of eye problems. His left eye had been injured many years ago and was shrunken and useless. His right eye had developed a cataract, so he was essentially blind. Last week the right eye suddenly became worse and the eye protruded. Apparently the globe (eyeball) had slightly popped out and the eyelids had slid behind it, trapping the eye in front of the lids. Infection developed and this was extremely painful. There was no saving the eye so the decision was made to remove it.
**WARNING!!!!!** If you're squeamish don't scroll down through the rest of the blog. I'm posting some pretty graphic images.
This is what the eye looked like just prior to surgery and after shaving and surgical prep. He is already under anesthesia at this point.
The cloudiness of the eye is a combination of cataract and pus. The dog was completely blind, so the eye was only causing discomfort. There was also severe damage to the eye so there wouldn't have been any benefit to putting it back into position. The surgery is actually not very difficult and can be done by most general practitioners. It's simply a matter of carefully cutting the muscles and connective tissues, gently freeing the globe from its attachments. After cutting the optic nerve at the back of the eye, the globe comes out easily.
The last photo is of the empty socket after the globe has been removed. The third eyelid and tear gland are removed and then the edges of the eyelid are cut away. The eyelids are sutured closed so that the socket and tissues are protected. In some cases a false eye is placed in the socket, but most vets don't do this and it is purely for appearances with no medical benefit. Here's a picture of the patient after the surgery was finished.
Dogs do quite well after the surgery and will go home with antibiotics and pain control. Sutures will come out in 7-10 days and by then they are usually back to normal. Since this kind of surgery is done because of severe damage to the eye, the dog is already blind prior to surgery, so removing the eye only improves their quality of life.
Who Knows Best?
A reader made this comment on another topic, and I thought it was worth addressing.
Except my vet doesn't think that I am smart enough nor know my pet well enough to hold it for him!!!Buddy, I know MY dog. And yes, he might snap. I'm no pushover, if you know what's best for you, you'd best let me doing the holdin'!
Not to be rude, but this is absolutely the wrong attitude to have. Most veterinarians won't let owners hold their pets because of safety, not because we don't think an owner is smart enough. In fact, I will generally refuse to see an aggressive pet if the owner won't let us restrain.
There are certain ways to properly hold a pet, and certain ways not do. This is important for the safety of the pet as well as the safety of anyone around them. If a person isn't restraining properly both that pet and anyone nearby could be injured, potentially even severely. Veterinarians and their staff undergo training to use proper restraint techniques and have extensive experience. When one of my staff isn't doing proper restraint, I'll work on correcting them, and all of my experienced staff are extremely good at safely keeping pets from harming anyone. I'm sorry for any hurt feelings, but very few pet owners have this kind of training.
Now this isn't true of all pet owners. I do have some that I will allow to do part of the restraint. However those are the exception rather than the rule, and if the pet is really trying to bite or scratch I'm going to trust my staff far more than I'm going to trust a client. And if it means losing that client because they won't let us do the restraint, I'll wave bye to them as they leave.
Besides safety, there is a major liability issue for the vet. People have sued and won because they were injured by their own pets during a veterinary visit. And don't say "well, I wouldn't sue if that happened." I have read reports from the AVMA liability insurance where a client would refuse to let the veterinary staff hold their pet and insist on doing it themselves even knowing the risk. The pet then injured the client (despite warnings from the vet) and the client turned around and sued the vet because the vet should have known better and not let them do it. I've seen examples of this numbers of times, so it wasn't an isolated incidence. I'm not willing to risk my license and my livelihood to prevent someone's hurt feelings.
So if you come into my office and your pet might bite, be prepared to let us hold it.
Except my vet doesn't think that I am smart enough nor know my pet well enough to hold it for him!!!Buddy, I know MY dog. And yes, he might snap. I'm no pushover, if you know what's best for you, you'd best let me doing the holdin'!
Not to be rude, but this is absolutely the wrong attitude to have. Most veterinarians won't let owners hold their pets because of safety, not because we don't think an owner is smart enough. In fact, I will generally refuse to see an aggressive pet if the owner won't let us restrain.
There are certain ways to properly hold a pet, and certain ways not do. This is important for the safety of the pet as well as the safety of anyone around them. If a person isn't restraining properly both that pet and anyone nearby could be injured, potentially even severely. Veterinarians and their staff undergo training to use proper restraint techniques and have extensive experience. When one of my staff isn't doing proper restraint, I'll work on correcting them, and all of my experienced staff are extremely good at safely keeping pets from harming anyone. I'm sorry for any hurt feelings, but very few pet owners have this kind of training.
Now this isn't true of all pet owners. I do have some that I will allow to do part of the restraint. However those are the exception rather than the rule, and if the pet is really trying to bite or scratch I'm going to trust my staff far more than I'm going to trust a client. And if it means losing that client because they won't let us do the restraint, I'll wave bye to them as they leave.
Besides safety, there is a major liability issue for the vet. People have sued and won because they were injured by their own pets during a veterinary visit. And don't say "well, I wouldn't sue if that happened." I have read reports from the AVMA liability insurance where a client would refuse to let the veterinary staff hold their pet and insist on doing it themselves even knowing the risk. The pet then injured the client (despite warnings from the vet) and the client turned around and sued the vet because the vet should have known better and not let them do it. I've seen examples of this numbers of times, so it wasn't an isolated incidence. I'm not willing to risk my license and my livelihood to prevent someone's hurt feelings.
So if you come into my office and your pet might bite, be prepared to let us hold it.
Updating
This past month I put up a non-veterinary poll out of curiosity. Though I don't get paid for this blog, I try to update frequently to keep people interested. However, since I don't get paid I also sometimes don't feel much motivation to post daily. For the most part this is done for fun and not profit. Even so, I know there are some regular readers and I don't want to disappoint too much. So how often do people like their blogs to update? Based on the results, fairly frequently!
Daily--35%
2-3 Times Weekly--52%
Weekly-9%
2-3 Times Monthly--3%
Once Monthly--0%
Most months I average around a post every other day, so it looks like I'm keeping it in the area of the top two choices. Obviously the more important part is that the posts are entertaining and informative, rather than just frequent. Quality is better than quantity.
A few more stats about the site. A year ago I started tracking hits to the blog. In that time there have been over 30,000 individual views, which has averaged to around 84 visits per day. There are also 25 regular followers. The blog has been read by people on every continent except Antarctica and in every hemisphere. I find all of that interesting for a small-time blogger like myself.
So thanks to everyone for reading the blog. Since I want this to be interactive, I'm always open to suggestions of topics and get excited when I get questions from readers.
Daily--35%
2-3 Times Weekly--52%
Weekly-9%
2-3 Times Monthly--3%
Once Monthly--0%
Most months I average around a post every other day, so it looks like I'm keeping it in the area of the top two choices. Obviously the more important part is that the posts are entertaining and informative, rather than just frequent. Quality is better than quantity.
A few more stats about the site. A year ago I started tracking hits to the blog. In that time there have been over 30,000 individual views, which has averaged to around 84 visits per day. There are also 25 regular followers. The blog has been read by people on every continent except Antarctica and in every hemisphere. I find all of that interesting for a small-time blogger like myself.
So thanks to everyone for reading the blog. Since I want this to be interactive, I'm always open to suggestions of topics and get excited when I get questions from readers.

